Dental Cleaning vs. Dental Deep Cleaning: Which One Do You Need?
Regular dental cleaning (prophylaxis) and dental deep cleaning (scaling and root planing) are distinct dental procedures with different goals: one prevents disease by removing plaque and tartar above the gumline, while the other treats established periodontal infection by debriding below the gumline and smoothing root surfaces. This article explains how each procedure works, the clinical signals that trigger a deep cleaning, and practical guidance on what to expect before, during, and after treatment. Readers will learn measurable diagnostic criteria—such as periodontal pocket depth and bleeding on probing—how Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT decide between prophylaxis and therapeutic SRP, and the long-term maintenance steps that protect results. The guide also compares outcomes, highlights risks of untreated periodontitis, and provides transparent explanations of cost drivers and typical insurance behavior. Throughout, we use clinical concepts like plaque, tartar (calculus), gum pockets, and tools such as ultrasonic scalers and hand scalers to clarify decisions and prepare you for conversations with Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT.
What Is a Regular Dental Cleaning and How Does It Prevent Gum Disease?
A regular dental cleaning, or dental prophylaxis, is a preventive dental procedure that removes supragingival plaque and calculus and polishes tooth surfaces to reduce bacterial accumulation and gingival inflammation. Mechanistically, prophylaxis interrupts biofilm formation above the gumline, lowering bacterial load and reducing the host inflammatory response that leads to gingivitis; this prevention preserves periodontal attachment and alveolar bone support. Current research shows consistent professional cleanings plus daily home care significantly lower the progression from gingivitis to periodontitis, which is why routine cleanings remain a cornerstone of preventive dental care. Understanding the steps and tools used in prophylaxis clarifies why it is effective for healthy mouths but insufficient once subgingival biofilm and deep pockets develop.
What Are the Steps and Tools Used in a Regular Dental Cleaning?

A routine cleaning begins with an oral exam to assess soft tissues and identify supragingival deposits, followed by scaling and polishing that target visible plaque and tartar. Scaling often uses a combination of ultrasonic scalers to dislodge calculus and hand scalers for precise removal; polishing smooths enamel and reduces future plaque adhesion. The procedure typically ends with flossing and a fluoride application or topical polish to help remineralize early enamel defects and reduce sensitivity. These steps—exam → supragingival scaling → polishing → flossing—work together to lower bacterial burden and interrupt the plaque-to-gingivitis pathway.
Intro: The following list outlines the principal instruments used during a routine dental cleaning.
- Ultrasonic scaler: Vibrates to break up hard calculus and flush pockets of debris.
- Hand scalers and curettes: Allow targeted scraping of plaque and tartar from tooth surfaces.
- Polishing handpiece: Smooths enamel to reduce future plaque retention.
- Dental mirror and explorer: Provide visual and tactile assessment during cleaning.
These instruments combine to create a comprehensive preventive visit that reduces gingival inflammation and prepares patients for ongoing home care.
Who Should Get Regular Dental Cleanings and How Often?
Most adults benefit from regular dental cleanings every six months, a schedule that balances plaque accumulation rates with practical prevention to maintain gingival health and detect early disease. Patients with risk factors—such as smoking, poorly controlled diabetes, a history of periodontitis, immunosuppression, or heavy calculus formation—often need more frequent visits (every three to four months) to control biofilm and inflammation. Pediatric, geriatric, and pregnant populations may require individualized schedules based on clinical findings and systemic considerations; for example, pregnancy-associated gingivitis often warrants closer monitoring. Discussing personal risk factors with your dental hygienist or Dr. Richard Malek at The Harmony Dental Group in Norwalk, CT helps determine an appropriate recall interval that prevents progression to periodontitis.
When Is a Deep Dental Cleaning Necessary to Treat Gum Disease?
A deep dental cleaning—commonly called scaling and root planing (SRP)—is necessary when periodontal disease has advanced beyond reversible gingivitis and created subgingival calculus, inflammation, and attachment loss that cannot be managed with supragingival prophylaxis alone. Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT base the decision on objective measures such as probing depth (typically pockets ≥4 mm with bleeding on probing), radiographic signs of alveolar bone loss, clinical attachment loss, and persistent symptoms like halitosis or tooth mobility. Scaling and root planing targets subgingival biofilm and calculus to reduce microbial challenge and facilitate periodontal reattachment; referrals to a periodontist are appropriate for unresponsive cases, extensive bone loss, or complex anatomic considerations. Early therapeutic SRP reduces disease burden and can avert the need for surgical intervention when combined with proper maintenance.
What Symptoms and Signs Indicate You Need a Deep Cleaning?
Several symptoms and clinical signs indicate the need for SRP: bleeding during brushing or probing, deepened periodontal pockets (≥4 mm), gum recession with exposed root surfaces, persistent bad breath, and tooth mobility in more advanced cases. Objective measures—probing depth, clinical attachment level, and radiographic bone loss—guide the treatment plan and prioritize quadrants for SRP; for example, localized 4–5 mm pockets with bleeding are often managed with quadrant SRP. Red flags requiring prompt care include pus on probing, rapidly increasing pocket depths, or increasing tooth mobility, which suggest active infection and loss of attachment. Recognizing these signs early improves prognosis and narrows treatment complexity.
Intro: Key diagnostic indicators prompt Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT to select SRP over prophylaxis.
- Probing depth ≥4 mm with bleeding on probing: Suggests subgingival infection requiring debridement.
- Radiographic bone loss: Confirms periodontitis and helps stage severity.
- Persistent halitosis and gum recession: Clinical signs of ongoing periodontal disease.
These indicators, when present together, shift management from prevention to active periodontal therapy and inform the scope and urgency of treatment.
Periodontal Health Assessment: Probing Pocket Depth and Bleeding on Probing in Adults
This study was conducted on adult patients aged 35–60 years. Periodontal evaluation, including probing pocket depth (PPD) and bleeding on probing (BOP), was performed using a Williams's periodontal probe. Mean PPD and BOP scores were calculated for both groups. Smoking and periodontal disease severity, probing pocket depth and bleeding on probing, 2021
How Does the Deep Cleaning Procedure Work: Scaling and Root Planing Explained?

Scaling and root planing is a therapeutic two-part process: scaling removes subgingival calculus and biofilm from root surfaces, and root planing smooths the root to eliminate bacterial niches and encourage connective tissue reattachment. Scaling → removes → subgingival calculus is a simple semantic triple that captures the procedure’s intent, while root planing → smooths → root surfaces describes the healing-promoting action that reduces plaque retention. Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT use ultrasonic instruments for bulk debridement and hand curettes for tactile root smoothing; local anesthesia is commonly used to control discomfort, and treatment may be staged by quadrant across multiple visits. Adjunctive therapies—such as localized antimicrobials—may be applied selectively to improve microbial control, and close post-procedure monitoring determines whether further periodontal intervention is necessary.
Scaling and Root Planing: Diagnosis and Treatment Planning in Periodontal Therapy
The clinical practice of scaling and root planing (SRP) as the foundational component of periodontal therapy is well-established. Parameters utilized for disease diagnosis and treatment plan formulation encompass probing depth, attachment level, bleeding on probing, and radiographic bone loss. A re‐evaluation of scaling and root planing, 2021
What Are the Benefits of Deep Cleaning Teeth Compared to Regular Cleaning?
Deep cleaning provides therapeutic benefits that go beyond the preventive scope of routine prophylaxis: it reduces pocket depth, lowers microbial load beneath the gumline, diminishes gingival inflammation, and promotes partial reattachment of connective tissue to root surfaces. These biological effects translate into clinical improvements such as decreased bleeding on probing, reduced halitosis, improved comfort, and a lower risk of progressive bone loss and tooth mobility when paired with effective maintenance. Unlike routine cleanings that manage supragingival biofilm, SRP directly addresses the subgingival niche where pathogenic bacteria drive periodontitis; therefore, it is essential for disease control in affected patients. Sustained benefits rely on a structured periodontal maintenance schedule to prevent reinfection and preserve attachment gains.
How Does Deep Cleaning Help Stop Gum Disease Progression and Promote Healing?
Deep cleaning reduces bacterial burden below the gingival margin by debriding calculus and biofilm, which lowers inflammatory mediators in the tissue and allows healing of the periodontal sulcus. Removal of rough calculus and smoothing of roots eliminates microenvironments where biofilm persists, permitting gingival fibroblasts and epithelial cells to reestablish a healthier attachment interface. Clinically, reductions in pocket depth and bleeding on probing are measurable outcomes of successful SRP, and when combined with improved oral hygiene, the likelihood of disease stabilization increases. This therapeutic pathway—biofilm removal → decreased inflammation → connective tissue healing—explains why SRP is the standard non-surgical treatment for periodontitis.
Intro: Key clinical benefits of SRP compared to prophylaxis include measurable improvements in periodontal health.
- Pocket depth reduction: Lowers risk of deeper infection and bone loss.
- Decreased bleeding and inflammation: Improves oral comfort and aesthetics.
- Reduced risk of tooth loss: Preserves function and support when maintained.
These benefits highlight why deep cleaning is a disease-focused intervention that complements preventive measures for long-term oral health.
What Are the Long-Term Oral Health Benefits of Deep Cleaning?
When SRP is followed by an individualized periodontal maintenance schedule, long-term benefits include sustained pocket depth stability, reduced incidence of tooth loss, improved masticatory function, and better oral-health-related quality of life. For many patients, periodic maintenance visits every three to four months are recommended to monitor healing, remove recurrent subgingival deposits, and reinforce home care—strategies that reduce relapse risk. Emerging evidence also links periodontal stability to reductions in systemic inflammatory markers, supporting broader health benefits when oral disease is controlled. Ultimately, SRP is a pivotal step in a long-term disease-management plan that preserves dentition and function when adhered to with regular follow-up.
How Does Gum Disease Develop and Why Does It Require Different Cleaning Approaches?
Gum disease develops in a sequence driven by microbial biofilm accumulation and the host inflammatory response: plaque accumulation leads to gingivitis, which is reversible with cleaning and hygiene; untreated gingivitis can progress to periodontitis when subgingival biofilms promote connective tissue destruction and alveolar bone resorption. Because periodontitis involves bacterial colonization below the gumline and structural loss of attachment, it requires therapeutic approaches—like SRP and sometimes surgery—that target the subgingival niche rather than standard prophylaxis alone. Risk factors such as smoking, diabetes, genetic predisposition, and inadequate oral hygiene accelerate progression from gingivitis to periodontitis, underscoring the need to tailor cleaning approaches to disease stage and patient-specific risk profiles.
What Are Gingivitis and Periodontitis: Causes, Symptoms, and Stages?
Gingivitis is an inflammatory condition limited to gingival tissues, characterized by redness, swelling, and bleeding on brushing that is reversible with professional cleaning and improved home care. Periodontitis represents a deeper, destructive process with clinical attachment loss, periodontal pocket formation, and progressive alveolar bone loss; it is staged by severity and complexity to guide treatment planning. Causes include persistent plaque and calculus, with host factors modulating disease expression; symptoms progress from bleeding and tenderness to recession, mobility, and eventual tooth loss if unmanaged. Distinguishing the two conditions is critical because gingivitis responds to prophylaxis, while periodontitis requires therapeutic debridement and ongoing maintenance.
Intro: The following list summarizes major differences between gingivitis and periodontitis for quick clinical recognition.
- Gingivitis: Inflammation confined to gingiva; reversible with cleaning.
- Early periodontitis: Pocketing and mild bone loss; needs SRP.
- Advanced periodontitis: Significant attachment loss and mobility; may require surgery.
Understanding these stages informs the choice of cleaning approach and long-term management strategy.
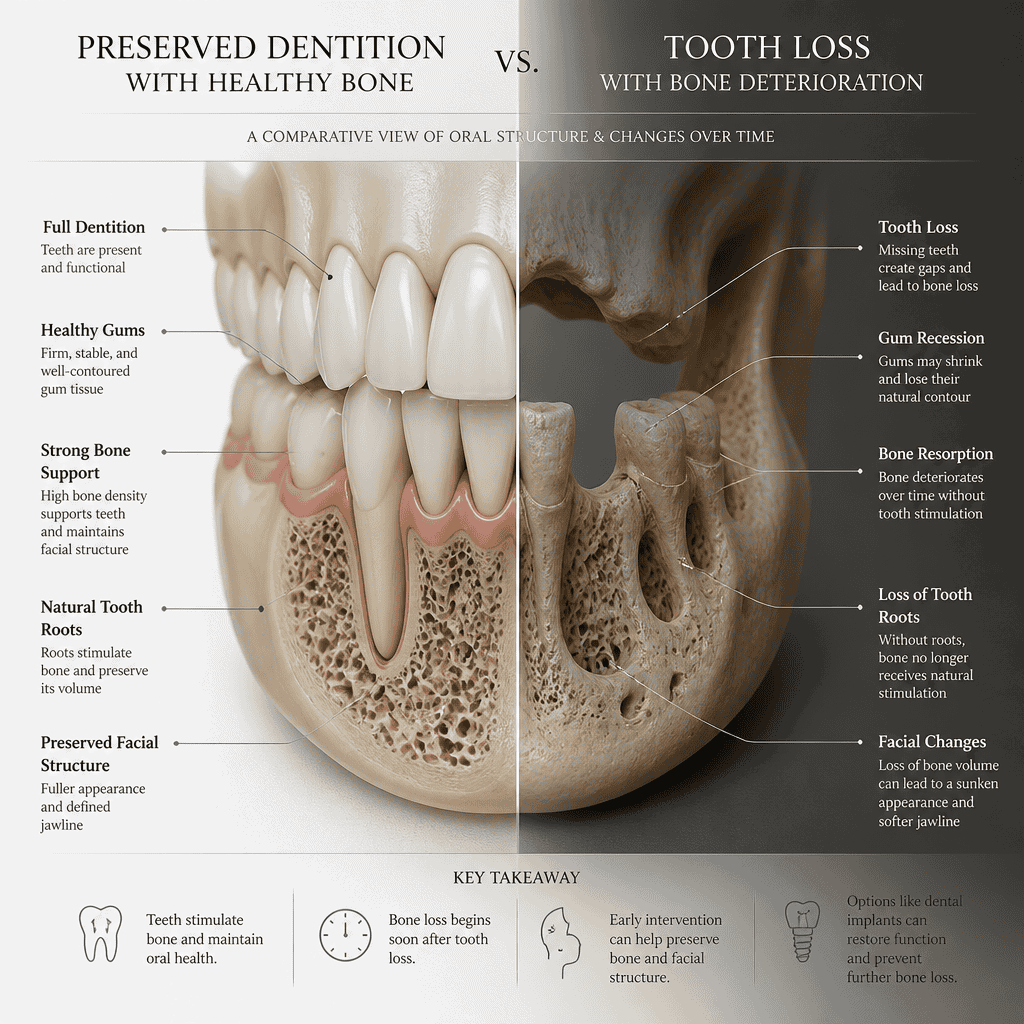
How Does Untreated Gum Disease Affect Your Teeth and Gums?
Untreated periodontitis leads to progressive connective tissue and bone destruction, resulting in increased tooth mobility, shifting dentition, and eventual tooth loss; these structural changes impair function and can necessitate complex restorative or replacement therapies. Beyond the oral cavity, chronic periodontal inflammation contributes to systemic inflammatory burden and is associated with adverse outcomes in patients with diabetes and cardiovascular conditions, making timely treatment clinically important. Functional consequences include impaired chewing efficiency and dietary limitations, while aesthetic and psychosocial impacts affect self-esteem and quality of life. Early intervention preserves both oral structures and overall wellbeing, demonstrating the broader value of appropriate periodontal therapy.
What Should You Expect During and After a Deep Dental Cleaning Procedure?
During a deep dental cleaning, expect a clinical protocol that may include local anesthesia, targeted subgingival scaling with ultrasonic and hand instruments, and root planing across affected quadrants; appointments may be staged over one or more visits depending on disease extent. Immediate common side effects include localized soreness, transient sensitivity, minor bleeding, and mild swelling; Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT typically recommend over-the-counter analgesics, cold compresses, and temporary adjustments to oral hygiene techniques to ease recovery. Post-procedure care often includes antimicrobial rinses, gentle cleaning methods, and a follow-up assessment to measure pocket-depth changes and healing; continued periodontal maintenance every three to four months is frequently advised to preserve therapeutic gains. Clear communication about expectations and a plan for pain and infection control reduces anxiety and improves adherence.
Is Deep Cleaning Painful and How Is Discomfort Managed?
Deep cleaning can cause discomfort if performed without anesthesia, but Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT commonly use local anesthesia to provide pain control during scaling and root planing, making the procedure tolerable for most patients. Discomfort after SRP tends to be mild to moderate and short-lived, managed with over-the-counter analgesics, topical gels, and cold therapy; prescription analgesics or sedative options are reserved for anxious or sensitive individuals. Proper anesthesia and pacing of appointments (e.g., quadrant-by-quadrant approach) reduce intraoperative and postoperative discomfort, and Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT provide specific instructions to minimize sensitivity during healing. Reassurance about predictable, controllable pain and a clear aftercare plan increases patient confidence and cooperation.
Intro: Below are common strategies used to manage pain and discomfort associated with SRP.
- Local anesthesia: Primary method to eliminate procedural pain.
- OTC analgesics and topical agents: Manage post-procedure soreness and sensitivity.
- Staged appointments: Reduce procedural time and improve comfort for extensive cases.
These management strategies make SRP an accessible and tolerable therapy for most patients when properly applied.
What Are the Aftercare Steps and Recovery Tips Following Deep Cleaning?
After SRP, patients should follow a recovery plan that emphasizes gentle oral hygiene, short-term dietary adjustments, and adherence to any antimicrobial rinse or medication prescribed to prevent reinfection and support healing. Recommended practices include soft foods for the first 24–48 hours, gentle toothbrushing with a soft brush, careful flossing once tolerated, and avoiding tobacco or alcohol that can impair healing; Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT may advise chlorhexidine or other antimicrobial rinses for a limited period. Scheduling a follow-up visit to reassess pocket depths and tissue response—typically within 4–8 weeks—helps determine if further therapy or referral is needed. Prompt reporting of severe pain, increasing swelling, or systemic signs of infection ensures timely management and protects treatment outcomes.
How Much Do Regular and Deep Dental Cleanings Cost and Are They Covered by Insurance?
Costs vary by region, provider, severity of disease, and number of quadrants treated: routine prophylaxis typically costs less than therapeutic SRP, while SRP pricing is often calculated per quadrant and increases with adjunctive procedures or specialist care. Insurance commonly treats prophylaxis as a preventive benefit, which may be fully or partially covered at regular intervals, whereas SRP is usually categorized as therapeutic periodontal treatment and may be subject to deductibles, frequency limits, or prior authorization requirements. Clear cost drivers include the number of quadrants requiring SRP, need for anesthesia or adjunctive antimicrobials, and whether a periodontist’s services are required. Patients are encouraged to verify benefit details, ask about codes used for claims, and discuss phased treatment plans with Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT to manage out-of-pocket costs.
What Factors Influence the Cost of Deep Cleaning and Regular Cleaning?
Several factors influence costs: the number of quadrants treated (SRP may be billed per quadrant), complexity and severity of periodontal disease, use of local anesthesia or sedation, Dr. Richard Malek or other periodontists at The Harmony Dental Group in Norwalk, CT, and adjunctive therapies such as local antimicrobials or systemic prescriptions. Geographic location and practice overhead also affect pricing; more extensive disease typically requires longer chair time and follow-up, increasing total expense. Example scenarios help illustrate cost drivers: single-quadrant SRP for limited pockets contrasts with full-mouth SRP staged across multiple appointments with adjunctive therapy and specialist care. Understanding these drivers allows patients to plan financially and discuss phased treatment when needed.
Intro: The cost comparison below shows typical cost components and example ranges per treatment scenario.
- Prophylaxis: Preventive cleaning with lower cost and frequent insurance coverage.
- SRP per quadrant: Higher cost due to therapeutic scope and often billed per quadrant.
- Adjunctives & specialist care: Increase total cost depending on need and provider type.
These categories clarify why SRP generally represents a greater expense than routine cleanings and why insurance handling differs between preventive and therapeutic codes.
How Does Dental Insurance Typically Cover These Procedures?
Dental insurance often covers routine prophylaxis as a preventive service with set frequency (commonly every six months), sometimes at little or no patient cost depending on plan details; in contrast, coverage for SRP is typically under therapeutic or major services and may require documentation of periodontal diagnosis, be subject to annual maximums, deductibles, and frequency limitations. Patients should request diagnostic records and treatment codes (e.g., periodontal charting, radiographs) to support claims and check whether preauthorization is necessary for SRP. When insurance coverage is limited, dental practices may offer phased treatment plans or financing options to spread costs while prioritizing urgent disease control. Verifying benefits in advance and coordinating with Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT can reduce unexpected out-of-pocket expenses.
Frequently Asked Questions
1. What is the difference between dental cleaning and deep cleaning?
Dental cleaning, or prophylaxis, is a preventive procedure that removes plaque and tartar from above the gumline, while deep cleaning, known as scaling and root planing (SRP), targets the subgingival area to treat periodontal disease. Prophylaxis is typically performed every six months, whereas SRP is necessary when gum disease has progressed, requiring more intensive treatment to remove bacteria and promote healing. Understanding this distinction is crucial for maintaining optimal oral health.
2. How can I tell if I need a deep cleaning?
Signs that you may need a deep cleaning include persistent bad breath, bleeding gums during brushing, and deepened periodontal pockets (≥4 mm). If you notice gum recession or tooth mobility, these are also indicators of advanced gum disease. Regular dental check-ups at The Harmony Dental Group in Norwalk, CT can help identify these symptoms early, allowing for timely intervention and treatment to prevent further complications.
3. What should I do to prepare for a deep cleaning appointment?
Before your deep cleaning appointment, inform Dr. Richard Malek at The Harmony Dental Group in Norwalk, CT about any medications you are taking and any medical conditions you have. It may also be helpful to maintain good oral hygiene leading up to the appointment. Arriving well-hydrated and relaxed can enhance your comfort during the procedure. Discuss any concerns with Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT to ensure you feel prepared and informed about the process.
4. How long does recovery take after a deep cleaning?
Recovery after a deep cleaning typically takes a few days. Patients may experience mild discomfort, sensitivity, or swelling, which can be managed with over-the-counter pain relievers. It's important to follow Dr. Richard Malek's aftercare instructions at The Harmony Dental Group in Norwalk, CT, which may include using antimicrobial rinses and avoiding hard foods for the first 24–48 hours. A follow-up appointment is usually scheduled within 4–8 weeks to assess healing and ensure the treatment was effective.
5. Can deep cleaning prevent future gum disease?
Yes, deep cleaning can significantly reduce the risk of future gum disease by removing harmful bacteria and promoting healing of the gum tissues. However, it is essential to follow up with a regular maintenance schedule, including professional cleanings and diligent home care practices. This proactive approach helps maintain periodontal health and prevents the recurrence of gum disease, ensuring long-term oral health.
6. Are there any risks associated with deep cleaning?
While deep cleaning is generally safe, some risks include temporary discomfort, sensitivity, and potential for infection if post-procedure care is not followed. In rare cases, patients may experience gum recession or changes in tooth sensitivity. Discussing any concerns with Dr. Richard Malek at The Harmony Dental Group in Norwalk, CT can help mitigate these risks and ensure a smooth recovery process.
7. How often should I have deep cleaning if I have gum disease?
The frequency of deep cleaning depends on the severity of your gum disease. Patients with mild to moderate periodontitis may require SRP every 3 to 4 months, while those with more advanced disease may need more frequent visits. Dr. Richard Malek at The Harmony Dental Group in Norwalk, CT will assess your condition and recommend a personalized maintenance schedule to effectively manage your periodontal health and prevent disease progression.
The Harmony Dental Group is a family-friendly dental practice in Norwalk, CT, led by Dr. Richard Malek, a former U.S. Air Force captain and experienced dentist with over 20 years of experience. Our team provides everything from routine cleanings and pediatric care to periodontal therapy, implants, and Invisalign. With the use of the latest laser technology, such as the FDA-approved Solea® laser, we offer gentle, precise treatment to help patients of all ages enjoy healthier gums, cleaner teeth, and confident smiles in a warm, welcoming environment.
To find out whether you need a regular cleaning or a deep cleaning, contact Dr. Richard Malek and his team at The Harmony Dental Group in Norwalk, CT today to schedule your appointment.